Smile Design & Aesthetic RehabilitationThe Complete Guide
- A smile makeover can restore confidence and function when planned with digital design, material selection, and conservative clinical execution.
Learn how world-class smile design works.
By Clinical Team · 8 Mar 2026 · 12 min read
Introduction: Beyond Cosmetic Dentistry
Aesthetic rehabilitation is not only about appearance, though that matters deeply to patients. The true goal is to improve harmony across gums, tooth proportions, smile line, and bite function while preserving healthy tooth structure and creating something that lasts decades.
For many patients, smile design also addresses confidence, speech comfort, and long-term oral maintenance. A poorly designed smile can create speaking difficulties, bite problems, and ongoing maintenance headaches. A well-designed smile works seamlessly.
World-class smile design combines clinical expertise, digital technology, and artistic vision. At India's top dental hospitals, the entire smile design process is handled by a specialist team: prosthodontists, periodontists, and cosmetic specialists working together from day one.
Questions about this procedure?
Digital Smile Design: The Technology That Changed Everything
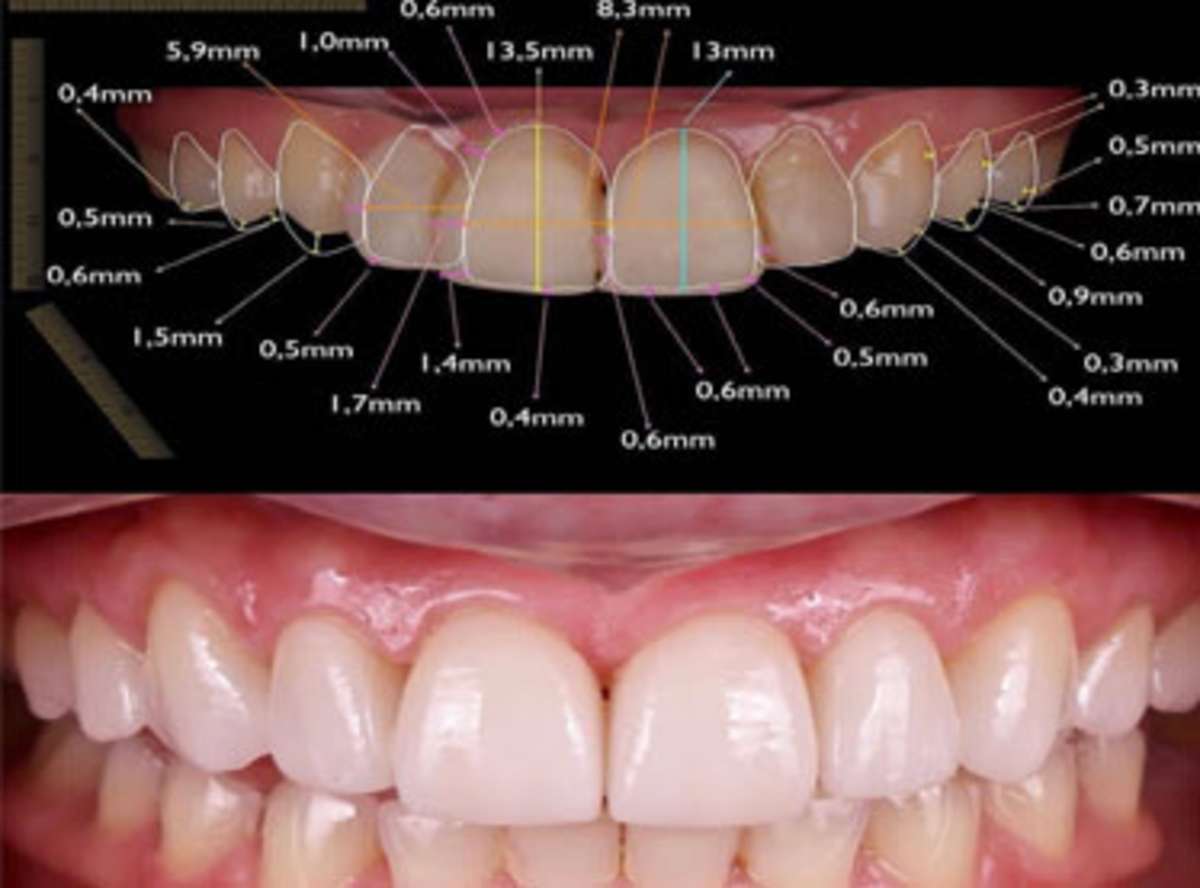
Digital Smile Design (DSD) is a software-based planning system that uses facial analysis, lip geometry, and tooth-to-face proportions to create a digital preview of your smile before any work begins. Instead of guessing what will look right, the team can show you exactly what the result will look like, with your unique face, your smile line, and your proportions.
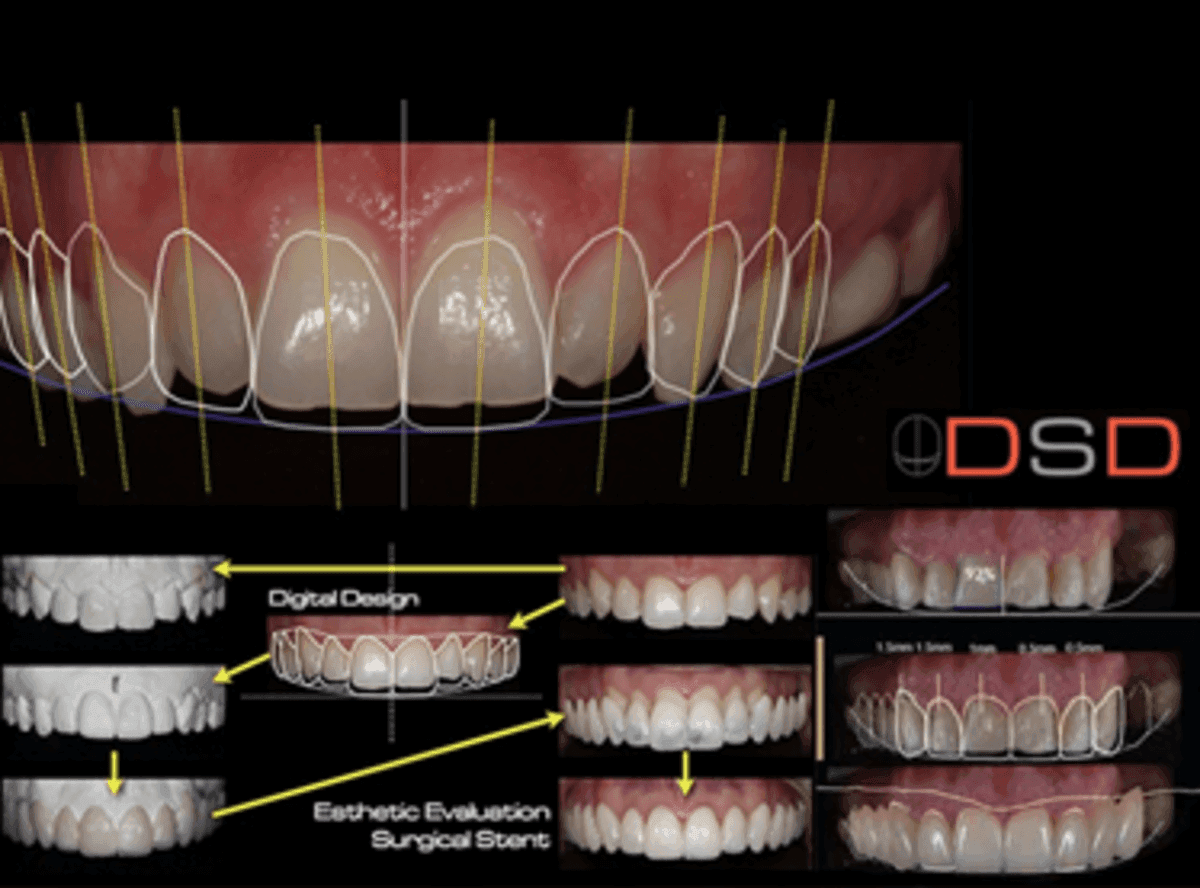
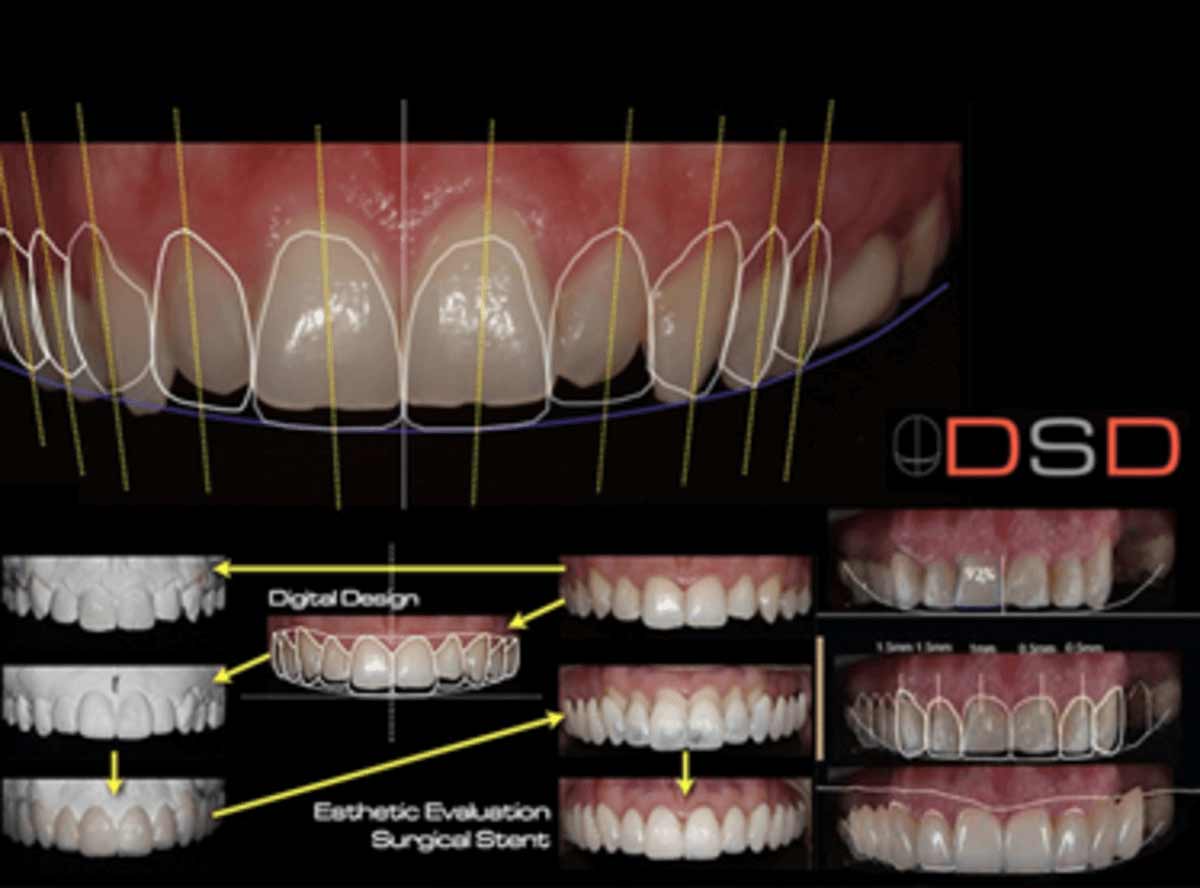
The process starts with standardized photography: frontal smile, relaxed, showing your natural dentition. The software then maps the key reference lines: the midline, the canine line, the smile arc, the buccal corridors, and the gum-smile relationship. Using these data points, the team creates a treatment-simulation layer that shows precisely what shade, shape, and contour will harmonize with your face.
This is not a guess. It is mathematics applied to aesthetics. Studies in leading dental journals show that DSD reduces treatment revisions by 70% compared to traditional analog planning. Patients see the plan before treatment begins, eliminating surprises.
At advanced clinics, DSD output feeds directly into CAD/CAM production systems, milling veneers or crowns with micron-level precision to match the digitally designed proportions.
Ready to discuss your options?
Veneer Systems: E-Max, Porcelain, and Composite Trade-Offs
Not all veneers are equivalent. The material choice depends on your enamel thickness, bite force, tooth structure, and aesthetic demands. Three systems dominate world-class smile design.
IPS e.max lithium disilicate is the gold standard. It is a crystalline ceramic that combines exceptional aesthetics with long-term durability. E-max veneers are ultra-thin (0.4-0.7mm), requiring minimal tooth preparation. They absorb light like natural enamel, creating depth and luminosity that other materials cannot match. They resist staining and last 15-25+ years in published follow-up studies. E-max is what Western cosmetic dentists choose for their own smiles because the aesthetic result is superior. The cost reflects that quality: $800-2,500 per tooth in Western clinics, $150-350 in India.
Traditional porcelain (feldspathic) veneers are slightly thicker and require more preparation. They are more forgiving if the preparation is imperfect, but they do not transmit light as naturally as e-max. They are falling out of favour in high-end cosmetic work because digital aesthetics have raised patient expectations.
Composite (resin) veneers are a direct placement option, no lab work, done in one appointment. They cost less and are easily repaired or adjusted. But composite veneers wear, stain, and discolour over 3-7 years. They are useful for small corrections or temporary solutions, not for comprehensive smile redesigns. Many patients using composite later regret not choosing e-max.
World-class smile design almost always means e-max because the investment in DSD, digital milling, and specialist time justifies premium material.
Curious about costs and timelines?

Gum Aesthetics and the Gum-Smile Relationship
A beautiful smile is 50% teeth and 50% gums. Many patients focus only on tooth colour and shape, ignoring the gum frame. A specialist smile design team does not make that mistake.
The gum-smile relationship is measured by three parameters: gum display, contour symmetry, and the interdental papilla architecture. Gum display refers to how much pink shows when you smile. The golden standard is 0-3mm of gum display above the teeth, any more and the smile looks 'gummy'; less and it can look short or mean.
Gum contour should follow the tooth anatomy: the interdental papilla fills the space between teeth (creating the 'contact point'), and the free gingival margin parallels the incisal edges. Asymmetrical gum contours or missing papillae are the first things cosmetic specialists notice in an unaesthetic smile.
At advanced clinics, gum reshaping using soft tissue lasers (diode, erbium, or CO2) creates ideal contours without scalpels or stitches. Laser gum contouring is precise, heals in 2-3 weeks with minimal pain, and creates a perfect frame for veneer or crown restorations. It is standard in high-end smile design but rare in many Western clinics because it requires specialized training.
Periodontists at top Indian hospitals perform gum design as part of the integrated smile design workflow, not as an afterthought.
Want a personalised treatment plan?

The Specialist Team Approach: Why One Doctor Is Not Enough
A comprehensive smile makeover requires multiple perspectives. If one dentist does everything, gum design, veneer prep, crown placement, shade selection, quality invariably suffers because no individual holds expertise in all domains.
India's top dental hospitals (17+ departments, 20+ surgical operatories) use a hub-and-spoke model: a prosthodontist leads the smile design, a periodontist handles gum architecture, a cosmetic specialist refines shade and contour, and if implants are needed, an implant surgeon joins the team. Each specialist reviews the case at key checkpoints.
This redundancy catches errors early. One specialist might miss a functional issue that another spots immediately. The prosthodontist might design the tooth shape, but the periodontist flags that the gum contour creates food traps, so the design adjusts. By surgery day, the plan has been pressure-tested by multiple experts.
At single-dentist clinics in Western countries, even experienced dentists cannot maintain this level of quality. The cost of having a periodontist, prosthodontist, and cosmetic specialist all on staff is prohibitive in most markets. India's specialist-dense hospital model makes this the default standard.
Questions about this procedure?
Material Selection Based on Your Bite and Esthetics
A beautiful material in the wrong bite environment will fail. Smile design requires matching material to mechanical reality.
If you have a heavy bite, grinding habit, or existing wear patterns, e-max veneers may be at risk. Some cases require full-coverage crowns instead, thicker, stronger, and capable of handling higher forces. A specialist team identifies this early using bite analysis tools like digital jaw tracking and static bite imaging.
If you have open contacts, misalignment, or a deep bite, some materials become impractical. A composite veneer in a deep-bite patient will chip at the incisal edge within months. E-max requires careful incisal contouring to avoid sharp edges that fracture under load.
Material selection also considers longevity goals. E-max is intended for 15-25+ year service life. Composite is 5-7 years. Zirconia crowns (used when more structure is needed) can last 20+ years but are more opaque than e-max, so they are reserved for cases where esthetics are secondary to strength.
Advanced clinics use computer analysis of bite forces and tooth stress distribution to model material failure risk before treatment begins.
Ready to discuss your options?

Conservative Preparation: Preserving Structure, Maximizing Longevity
Over-preparation is the enemy of longevity. Remove more tooth structure than necessary and you create pulp exposure risk, increase sensitivity, and reduce the veneer bond surface. The philosophy of modern cosmetic dentistry is: remove only what is necessary.
With e-max veneers, the preparation depth is typically 0.4-0.7mm on the facial surface, less than a millimetre of tooth removal. Compare that to traditional crowns, which require 1.5-2mm of removal. The difference is enormous for tooth longevity.
Preparation should also follow a systematic protocol: define the margins (supragingival is preferred, above the gum line, because it is easier to place, seal, and keep clean), avoid sharp internal line angles (they concentrate stress), and taper the preparation at a specific angle. Digital planning systems specify the exact preparation geometry before the dentist picks up a drill.
Some cases can be treated without preparation at all, direct bonded veneers or lumineers. These are possible only if the existing tooth surface is adequate. If teeth are severely rotated, sized, or shaded incorrectly, minimal-prep solutions cannot achieve the design goal. The specialist team will recommend either: (a) orthodontics first, then minimal-prep veneers, or (b) traditional-prep veneers for a faster result.
Curious about costs and timelines?
The Clinical Workflow: From Smile Design to Final Placement
Modern smile design workflow is sequential and non-negotiable. Deviating from it introduces errors.
Phase 1: Records and diagnosis. The team collects standardized photos (frontal, smile, lateral, intraoral), digital scans (3D of teeth and gums), and bite records. CBCT imaging is done if bone structure is a factor. From these records, the DSD plan is created and reviewed with the patient.
Phase 2: Patient approval and shade selection. Once the digital plan is approved, the team creates a shade guide mockup, temporary composite on the prepared teeth showing the planned result. This is your chance to see the design in your mouth before final restorations are made. Adjustments can still be made at this stage without penalty.
Phase 3: Tooth preparation. With the approved plan as a guide, the dentist prepares teeth using standardized burs and depth guides. Preparation is confirmed with depth gauges to ensure consistency.
Phase 4: Lab fabrication. Digital data (scan, design, preparation taper) goes to the in-house CAD/CAM lab, which mills restorations from an e-max block or fab works layered ceramics by hand. Colour stratification, margin contour, and incisal surface texture are controlled by the lab tech and prosthodontist.
Phase 5: Try-in and refinement. Restorations are tried in, margins are checked (should be invisible and smooth), contacts are verified, and function is tested. Shade is confirmed under natural and artificial light. Adjustments are made if needed.
Phase 6: Permanent cementation. Once approved, restorations are ultrasonically cleaned, the tooth is etched and primed, and the restoration is bonded with composite cement. Margins are polished and sealed. The restoration becomes part of the tooth.
Want a personalised treatment plan?
Aftercare and Long-Term Maintenance
A smile designed and placed with precision requires protection and maintenance to last 15-25 years.
Dietary discipline matters. Hard and sticky foods (ice, nuts, caramel, gum) stress veneer edges and can cause chipping or separation. While modern e-max is durable, it is not indestructible. Patients are advised to treat veneers like natural teeth, chew carefully.
A night guard is standard recommendation if you grind or clench. Bruxism can fracture veneers or cause micromotion at the margins, leading to staining and leakage. A custom guard costs $200-400 and prevents $3,000-5,000 in repairs.
Oral hygiene must be meticulous, especially at veneer margins. Biofilm accumulation can cause margin staining and gum inflammation. Electric toothbrushes and daily flossing are non-negotiable. Some patients switch to water flossers for easier access.
Professional reviews are scheduled every 6-12 months. The dentist checks for margin integrity, recurrent decay, gum inflammation, and any cosmetic drift. Small issues caught early cost $50-200 to fix; ignored, they cost $1,000+.
If a veneer ever fails, cracks, separates, or discolours beyond repair, it can be removed and replaced without affecting the underlying tooth. The investment in conservative preparation means that repair is feasible. If the tooth itself is healthy, a new veneer is simply bonded over the original preparation.
Questions about this procedure?

Cost and Timeline: What to Expect
A comprehensive smile makeover (16-20 veneers, gum design, full diagnostic imaging) costs $25,000-50,000 in Western countries and $3,500-6,000 in India, same materials, same technology, same specialist team.
Timeline in India is typically 7-10 days. Day 1-2: diagnostics, DSD planning, and patient approval. Day 3-4: shade mockup try-in and approval. Day 5-6: tooth preparation and initial lab fabrication. Day 7-8: try-in and refinement. Day 9-10: final cementation and departure. Some patients return for a final review appointment 3-4 weeks later, but the bulk of treatment is complete.
In Western countries, the same timeline is compressed across 3-4 weeks due to lab turnaround and appointment spacing. In India, dedicated in-house labs reduce turnaround to 24-48 hours, allowing treatment acceleration.
Tele-dentistry follow-ups at 2 weeks, 3 months, and 1 year are included in most packages. If issues arise, video consultation with the clinical team is immediate.
Ready to discuss your options?
Conclusion: Why Smile Design Is Worth the Investment
A smile makeover is one of the few medical-cosmetic investments that improves daily life for decades. When planned with digital precision, executed by specialists, and maintained with discipline, smile design delivers predictable, beautiful, long-lasting results.
The alternative, ad-hoc veneering by a generalist, or worse, DIY teeth whitening and off-the-shelf smile kits, is penny-wise and pound-foolish. Patients spend less money initially but end up with compromised aesthetics, functional problems, and costly repairs.
Investing in world-class smile design is investing in how you look and feel every day for 15-25 years. That is worth getting right from the start.
Curious about costs and timelines?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
What is Digital Smile Design and why does it matter?
Digital Smile Design (DSD) is a software-based planning system that uses facial analysis and digital tooth-mapping to show you exactly what your smile will look like before any treatment begins. It eliminates guesswork and reduces treatment revisions by 70% compared to traditional planning. You approve the design with your face in it before the dentist picks up any instruments.
What is the difference between e-max, porcelain, and composite veneers?
E-max (lithium disilicate) is the gold standard, ultra-thin (0.4-0.7mm), most natural-looking, resistant to staining, and lasts 15-25 years. Porcelain is thicker and less aesthetic. Composite (resin) is inexpensive but wears and discolours in 3-7 years. World-class smile designs almost always use e-max because the investment justifies premium material.
Do veneers require a lot of tooth preparation?
Not anymore. Modern e-max veneers require only 0.4-0.7mm of preparation, less than a millimetre of tooth removal. This is far less than crowns. Some cases can be treated with minimal-prep or no-prep veneers if the tooth surface is already well-shaped.
How important is gum design in a smile makeover?
Very important. A beautiful smile is 50% teeth and 50% gums. Gum display, contour symmetry, and interdental papilla architecture are critical. Specialist cosmetic dentists use soft tissue lasers to reshape gums as part of the integrated smile design, something that is standard in world-class clinics but rare elsewhere.
Why do I need multiple specialists for a smile makeover?
A prosthodontist handles tooth design, a periodontist designs gum architecture, a cosmetic specialist refines shade and contour, and an implant surgeon steps in if implants are needed. Each specialist reviews the case and catches errors early. Quality improves when multiple experts are involved.
How long do smile makeovers last?
Modern e-max veneers last 15-25 years with proper care. Longevity depends on the material (e-max lasts longer than porcelain or composite), the quality of preparation and placement, your bite and habits, and your maintenance (night guard if you grind, careful diet, and professional reviews every 6-12 months).
What happens if a veneer cracks or discolours?
If a veneer fails, it is removed and replaced without affecting the underlying tooth, because conservative preparation was done initially. The new veneer is simply bonded over the original preparation. This is why conservative dentistry is so important: it preserves options for the future.
How much does a smile makeover cost in India vs Western countries?
A comprehensive smile makeover (16-20 veneers, gum design) costs $25,000-50,000 in Western countries and $3,500-6,000 in India. Same materials, same technology, same specialists. The savings come from lower lab and clinic costs, not lower quality.
How long does a smile makeover take?
In India: 7-10 days (diagnostics, DSD planning, shade mockup, preparation, try-in, final placement). In Western countries: 3-4 weeks across multiple appointments due to lab turnaround. India's in-house labs accelerate treatment.
What should I do after my smile makeover is complete?
Maintain strict oral hygiene, use a night guard if you grind, avoid hard and sticky foods, attend professional reviews every 6-12 months, and use a custom-fit mouth guard during sports. These steps ensure your veneers last 15-25 years.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










