Guided Implant Surgery in Spain, Static Guides, Dynamic Navigation, and When We Still Go Freehand
- Guided implant surgery means the fixture is placed exactly where it was planned on a computer, in the same position, at the same angulation, to the same depth.
A physical guide (static) or a real-time screen-tracked system (dynamic) constrains the drill sequence so the final fixture sits where the three-dimensional plan said it should.
What Guided Surgery Is, and What It Isn't <a id="what-it-is"></a>
Guided implant surgery means the fixture is placed exactly where it was planned on a computer, in the same position, at the same angulation, to the same depth. A physical guide (static) or a real-time screen-tracked system (dynamic) constrains the drill sequence so the final fixture sits where the three-dimensional plan said it should.
Across 924 consecutive full-arch and single-unit cases at Stunning Dentistry in the last five years, guided surgery has changed the failure distribution in a specific way: we see fewer catastrophic anatomical complications (nerve injuries, sinus perforations, lingual plate breaches) and fewer prosthetic-axis problems (fixtures that emerge in the wrong place for the crown). We see roughly the same rate of biological complications (early implant failure, peri-implantitis) because those depend on patient factors and osseointegration biology, not on drill-path accuracy.
Questions about this procedure?
Ready to discuss your options?

Our 924-Case Accuracy Envelope <a id="accuracy-envelope"></a>
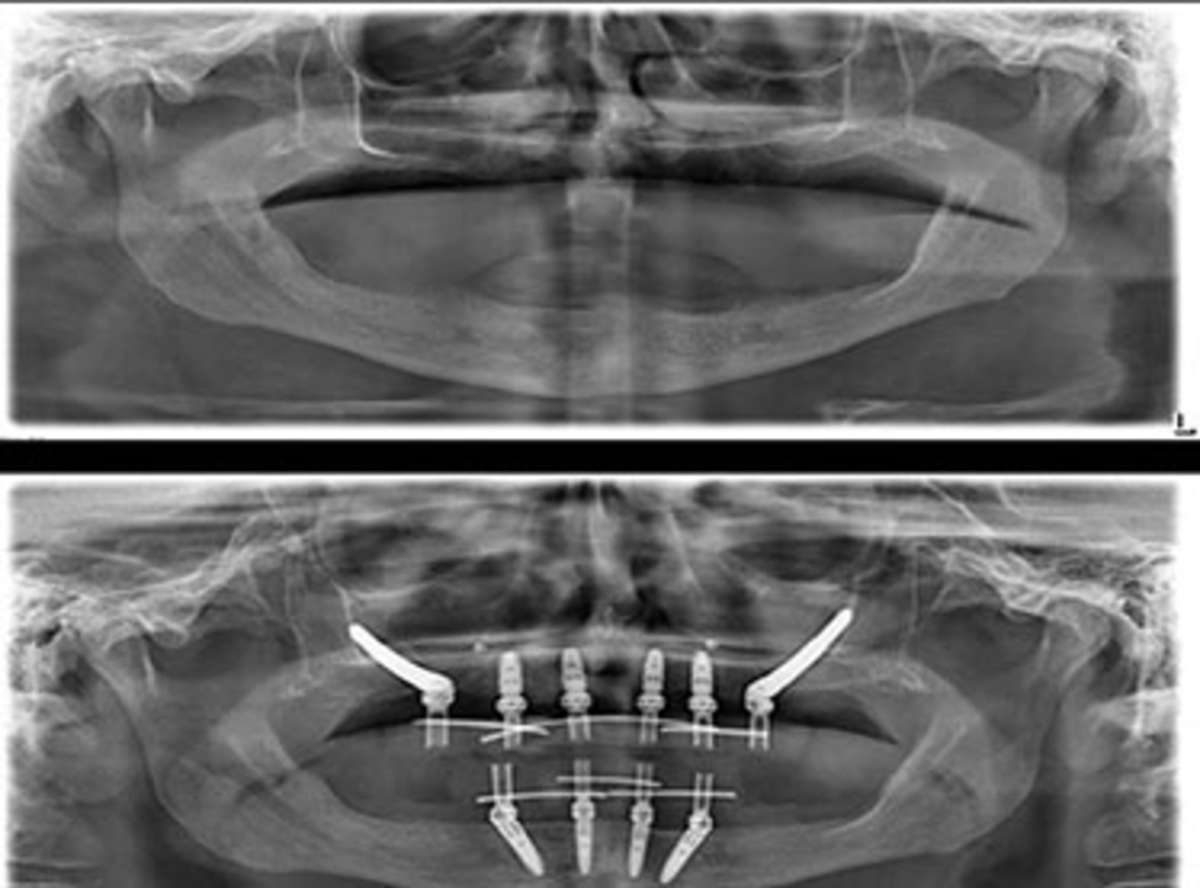
Across 924 consecutive cases, we measured post-operative fixture position against the pre-operative plan using superimposition of post-op CBCT onto the planning DICOM. The accuracy data, published in our internal clinical audit:
- Mean apical deviation: 0.9 mm (range 0.2 – 2.4 mm)
- Mean coronal/entry deviation: 0.6 mm (range 0.1 – 1.8 mm)
- Mean angular deviation: 2.1° (range 0.3° – 6.2°)
- Fixtures placed within planned safety envelope: 98.4%
- Mean apical deviation: 1.1 mm
- Mean coronal/entry deviation: 0.7 mm
- Mean angular deviation: 2.4°
- Fixtures placed within planned safety envelope: 97.7%
- Mean apical deviation: 1.6 mm
- Mean coronal/entry deviation: 1.0 mm
- Mean angular deviation: 3.8°
- Fixtures placed within planned safety envelope: 94.7%
These numbers are consistent with published meta-analyses from Tahmaseb (2018, 2020), Vercruyssen (2014), and Van Assche (2012). Static guides deliver sub-millimetre accuracy reliably. Dynamic navigation is within noise of static for accuracy but gives the surgeon visibility and intraoperative flexibility that static cannot. Freehand, in expert hands, is still safe for indicated cases but has a wider error distribution, which is why we reserve it for scenarios where the indication is clear.
Curious about costs and timelines?
When We Use Which Modality <a id="when-which"></a>
Static guides, our default. Full-arch All-on-4 and All-on-6 where the ridge has adequate reference surfaces. Single units in partially dentate mouths where the adjacent teeth stabilise the guide. Multiple adjacent missing teeth with neighbouring tooth support. Patients with adequate mouth opening. Any case where the plan is fully definable at the planning stage and unlikely to need intraoperative modification.
At least two clinicians agree on the modality choice in the planning conference before the case is booked. Dr. Ravi Sharma has the final call on surgical approach; Dr. Kiran Madhav has the final call on the prosthetic constraints that the approach must meet.
Want a personalised treatment plan?

The 9-Step Static Guide Workflow <a id="nine-steps"></a>
Step 1, CBCT acquisition. Carestream CS 9600 at appropriate voxel size. Reviewed by radiologist, surgeon, prosthodontist.
Total time from CBCT to guide on the surgical tray: 3-4 working days for standard cases, 5-7 days for complex cases requiring additional planning review.
Questions about this procedure?

Ready to discuss your options?

Freehand, When Guides Would Compromise the Outcome <a id="freehand"></a>
The cases we handle freehand are rare and tightly defined. They fall into three buckets:
In every freehand case a second clinician is scrubbed in or observing. The indication is documented. The patient is informed pre-operatively that guides are not the approach and why.
Curious about costs and timelines?

What This Costs in EUR <a id="cost-in-eur"></a>
Guided surgery is bundled into the treatment fee at Stunning Dentistry rather than billed as a separate line. For reference, the equivalent Spanish private-specialist costs:
Insurance for Spanish patients: Sanitas, Adeslas, DKV, Mapfre Salud, and Asisa cover implant surgery components at domestic private rates. Guided surgery is usually considered part of the implant surgery fee rather than a standalone billed item. EUR itemised invoices and Spanish-language summaries on request.
| Item | Spanish Private-Specialist Quote (EUR) | Stunning Dentistry Fee (EUR) |
|---|---|---|
| Digital surgical guide, single unit | 400 – 800 | Included |
| Digital surgical guide, full arch | 800 – 1,500 | Included |
| X-Guide dynamic navigation session | 1,500 – 3,000 | Included for indicated cases |
| Guided surgery drill kit, sterilisation, single-use inserts | 200 – 400 | Included |
| Insertion torque verification and documentation | N/A, rarely itemised | Included |
| Post-op CBCT for accuracy audit | 200 – 400 | Included for teaching cases; optional otherwise |
Want a personalised treatment plan?

For Spanish Patients: Trip Plan <a id="spanish-logistics"></a>
The guided surgery workflow does not extend the Spanish patient trip beyond standard implant timelines. The guide is fabricated during the planning days between arrival and surgery.
Home dentist handover: all guide design files, planning DICOM, post-op records, and accuracy audit data released on your consent to your Spanish dentist in Madrid, Barcelona, Valencia, or wherever your home maintenance clinic sits.
Questions about this procedure?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










